Whether it’s on your back, your side or on all fours, there are positions to take… and some things to know.
Contractions
Contractions occur when the uterine muscles tighten and relax in a continuous motion as your body prepares to birth your baby. In the earlier stages of labour, contractions are likely to be irregularly timed, short and sharp. They can be anywhere from 45 minutes (or less) to hours apart, each lasting around 20-30 seconds.
Generally speaking, when your contractions become strong, painful to the point you may be unable to speak, 45-60 seconds each and they've occurred five minutes apart for around an hour, it's a good sign to make contact with your birth team. Grab your hospital bag as it's likely to be 'go time'! Like everything else, if you're in doubt or confused whether to stay at home or go into hospital - always call your team to be safe.
Dilation
Whether in the movies or in pregnancy books, we've all heard about the phrase '10cm dilated!" Dilation refers to the size of the cervix opening, where your baby will come out. Your cervix is continuously checked during the early stages of labour by your midwife via a vaginal examination (with your consent). The reason being; the size of the cervix opening is a good indication of the progression of your labour.
The time it takes to dilate is different for all women. It can take hours or minutes to move from one stage to the next.
Bring in pain relief
The hospital will have medical pain relief available should you need it. These will have varying effects on you and sometimes your baby so it is important to understand them and their effects. As way of introduction, these include;
- Nitrous oxide. Also known as ‘laughing gas’ or just ‘gas’. It is administered through a face mask or tube held at the mouth. It takes a few seconds to be felt so for it to be effective you must breathe from it as soon as a new contraction starts. It will not completely block the pain but will dull the intensity.
- Pethidine. A strong pain reliever related to morphine which is usually injected into a muscle or given intravenously (into a vein). It usually lasts 2-4 hours and is given with anti-nausea medication to mitigate side effects of feeling sick.
- Epidural anaesthesia. The most effective pain relief available, it numbs feeling from the waist down via an injection into the spinal cord through the back. It is available for vaginal births and used in caesarean births because it allows the mother to stay awake and alert during the baby's birth. It is always accompanied by a urinary catheter and often a further mode of monitoring the baby’s heart. A It can take some time after delivery for the numbness to go away, so you may be confined to bed for the rest of the day.
You may like to consider bringing in some other non-medical pain relief options from home. These may include;
- A heat pack for your lower back
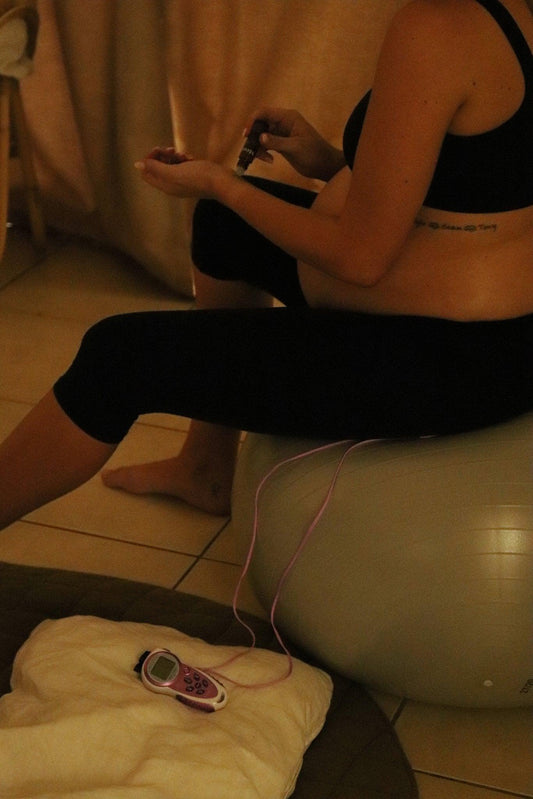
- A TENS machine. A TENS machine is attached to your back with sticky pads and its job is to send electrical impulses to certain parts of the body to block pain signals.
- Soothing music for distraction
- Magnesium oil to rub into your lower back, helping any strained muscles to relax
- Your partner or doula for massage
- Pushing or bearing down
As your labour progresses and your baby's head lowers, this will place pressure on your lower pelvis. At this point, many women feel a very strong urge to push or poo. The latter is totally normal, it's a common sign of birth approaching! Despite your body's instinctive response (to push), it's important to communicate with your birthing team before doing so.
The reason for this is that you might not actually be 10cm dilated yet and as your body is still contracting, there are certain times when pushing is optimal and certain times when pushing is not. Follow the guidance from your birth team to help you find a nice rhythm while also lowering the risk of tearing or other pelvic floor damage.
Bring in assistance
Forceps and a ventouse are instruments that protectively hold or suck onto the baby’s head, allowing the birth team to gently (and safely) pull and assist your baby through the birth canal and then through the vagina.
Examples of when your birth team may opt to use either of these tools for assistance include (but are not limited to);
- If after a certain duration of pushing, the baby is having trouble coming through the birth canal
- If there are concerns for the baby's heart rate or if the baby is showing signs of fatigue or distress
- If the baby has wriggled or turned into an 'awkward' potion making it harder for you to push them out
- If you are showing signs of fatigue or;
- If you have pre-existing medical conditions that have to be considered (i.e. previous heart issues)
 Mid Season Sale
Mid Season Sale